Lecture Notes, Biology 203, Human Sexuality and Reproduction
Contraception, Sterilization and Abortion, Part 3
- Progestin-only contraceptive pills (mini-pills), implants (Norplant), injections (Depo-Provera)
- Do not work by inhibiting ovulation only (40-65% ovulate, 15-40% don't ovulate, 20% shift between cycles)
- Progestins alter characteristics of endometrium, ovum transport, etc.
- Safe for nursing mothers
- Irregular or skipped menstruation can be disconcerting for some women
- Pills must be taken every day at same time (chance of pregnancy due to missing a pill is greater than with combined BCP's)
- Injections (DepoProvera) are given every three months, with a 4-6 week grace period in which to make appointment, average time to conception 6 months)
- Implants (Norplant) (6 implants in arm release progestins slowly over 5 years before must be removed, cost $500-700 to insert, average time to conception 1 month)
- Sterilization
- Should be regarded as permanent--procedures not always reversible
- In both sexes, consist of blocking tube (Fallopian tube or vas deferens) to prevent contact between egg and sperm
- Men: vasectomy
- Usually one or two small incisions through scrotum to reach vas deferens on both sides
- Usually loop tied off and removed (procedure)
- Done in doctor's (urologist, usually) office with local anesthetic in about 20 minutes
- No heavy lifting for 48 hours, tylenol with codeine for pain, one week recovery time
- No risk of impotence or reduced sex drive
- Not sterile immediately--requires 10 ejaculations and then a sperm count to make sure there are no sperm in semen
- 1/2 to 2/3 of men develop anti-sperm antibodies, with no particular consequences
- May be reversible, by a good microsurgeon: anatomical success 40-90%, clinical success (pregnancy) 18-60%
- One study done in small number of monkeys about 20 yrs. ago showed a slight increase in risk of cardiovascular disease
- No risk of death associated with vasectomies (no general anesthetic, no entry into abdominal cavity)
- Women: tubal ligation
- Block Fallopian tubes with ligation, clips, rings, electrocoagulation (procedure)
- Usually done using laparoscope to visualized area and perform ligation (one or two small incisions through abdominal wall)
- Done as outpatient in clinic or hospital
- More risky than vasectomy because often uses regional or general anesthetic, and involves entry into abdomen
- More expensive than vasectomy
- Might be reversed by microsurgeon--anatomical success 50-70%, clinical success (pregnancy) 10-50%
- Women: hysterectomy
- Should not be done just for sterilization--too risky, major surgery
- If ovaries removed as well as uterus, lack of estrogen/progesterone will cause early menopause
- Induced abortion
- If a pregnancy is unwanted, the woman has many choices to make:
- She can have the baby and keep it.
- She can have the baby and give it up for adoption.
- She can abort the pregnancy.
- Goal of induced abortion is to remove the products of conception--all embryonic/fetal tissue, including chorionic villi/placenta
- Most abortions induced during first trimester (1st 13 weeks) (50% less than 8 wks, 89% less than 13 weeks)
- Almost all the rest induced during second trimester (14-24 weeks) (only 1% after 20 weeks)
- Risk of death and complications increases with duration of pregnancy, mostly due to type of procedure used for the abortion (see table)
- Early medical methods (see table)
- RU-486 (mifepristone) given as pills, induces contractions that expel embryo/fetus in 2 days
- Methotrexate/misoprostol given as vaginal suppository induces contractions in 5-7 days
- Act as anti-progesterones plus prostaglandins
- Used in the first to 7th weeks of pregnancy
- Effective in 95-6% of women
- Complications: one in 8-10 women have week-long uterine bleeding, rarely nausea or diarrhea
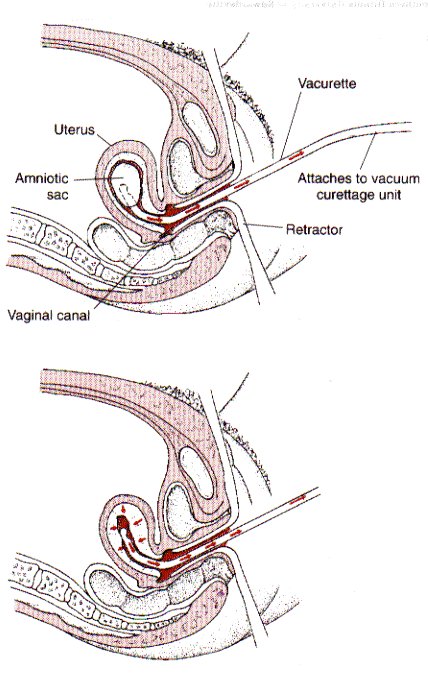
- Vacuum curettage
- Surgical procedure used from 1st to 13th weeks (most common abortion method)
- Requires local anesthetic
- Dilation and extraction
- Surgical procedure used from 13th to 16th weeks
- Fetus larger, may require larger curette to remove tissues
- May use oxytocin to induce contractions, reduce bleeding
- After 20th week, use intact dilation and extraction--more like induced labor, more risky (rare)
- Complications: bleeding, cramping, pain, infection (fever, foul vaginal discharge), urinary problems, depression
- Rh negative women should have Rhogam shot to prevent Rh disease in subsequent pregnancies
- Women may benefit from counseling after abortions
- After 2-4 weeks, woman should have pelvic exam to make sure healing is progressing with no sign of infection
- Woman should avoid intercourse for two to three weeks, and use some form of contraception
- In consultation before abortion, counselor should gather information about menstrual history, reproductive history, allergies, acute/chronic illnesses, pregnancy test, Rh typing, diagnostic tests for STD's
- In decade following legalization of abortion (1973), maternal mortality, infant mortality and premature births were all reduced--leveled off since 1985
- Many states have introduced legislation to restrict women's choice in various ways
- Women choose to abort pregnancies whether legal or illegal--fewer women die from legal abortions than illegal ones.
- Never a trivial decision, and hard to be sure of choice until person is in the situation of an unwanted pregnancy
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}